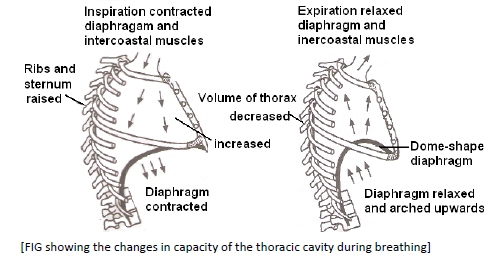
i) Diaphragm: When relaxed the diaphragm is dome-shaped structure which separates the thoracic cavity from the abdominal cavity. Phrenic or radial muscles extened from diaphragm to ribs and vertebral column. When these muscles contract diaphragm becomes flat, thus increases the thoracic cavity antero posteriorly. These are the principle inspiratory muscles and play about 75% role in inspiration, other muscles play 25% role in inspiration.
ii) External intercoastal muscles: They occur between the ribs. These are 11 pairs of muscles extending between 12 pairs of ribs. Their contraction pulls the ribs and sternum upward and outward there by increasing the thoracic cavity dorso-ventrally
and laterally.
iii) Abdominal muscles: These muscles relax and allow compression of abdominal organs by diaphragm.
EXPIRATION
• It is the process by which foul air is expelled out of the lungs. Expiration is normally a passive process and involves the relaxation of inspiration, expiratory muscles becomes active, making expiration an active energy consumed process
i) Diaphragm: When muscles of diaphragm relax it again becomes dome-shaped, decreasing the thoracic cavity.
ii) External intercoastal muscles: When these muscles relax, sternum and ribs come to their original position. This also decreases thoracic cavity.
iii) Abdominal muscles: Contraction of abdominal muscles presses the abdominal viscera against the diaphragm, bulging it further upward and thus decreasing the thoracic cavity more vertically.
iv) Internal intercoastal muscles: Contraction of these muscles moves the ribs downward and inward and reduces the thoracic cavity laterally and dorsoventrally. The abdominal and external intercoastal muscles are called expiratory muscles.
• Due to the action of above muscles, the overall volume of thoracic cavity decreases and the intra pleural pressure increase by +3 to +4 mmHg. Due to this increased pressure in lungs, foul air is given out of them.
• One breath includes one inspiration and one expiration.
• The respiratory rate is the number of breaths taken per minute. For a person breathing normally at rest, it is equal to 12-14 breath per minute.
• Breathing through nose is healthier as it get filtered and conchal of nose warm up the air.
• Mammals have a negative pressure breathing as it allows them to eat and breath at the same time and in human female thoracic breathing is more predominant.
PULMONARY AIR VOLUMES AND CAPACITIES
• Spirometry is the process of recording the changes in the volume movement of air into and out of lungs and the instrument used for this purpose is called sphirometer or respirometer. The graph showing the changes in the pulmonary volumes and capacities under different conditions of birthing is called spirogram.
• The quantity of air the lungs can receive, hold or expel under different conditions are called pulmonary volumes.
• Combinations of two or more pulmonary volumes are called pulmonary capacities.
• Tidal volume (T.V.): Volume of air inspired or expired in relaxed or resting position -500ml. It consists of 150 ml of dead space volume and 350 ml of alveolar volume.
• Dead space: Part of inspiratory tract not involved in gaseous exchange. ( Nose to terminal bronchi, volume 150 ml)
• Residual volume (R.V): Air left in lungs and dead space after forceful expiration. 1.1-1.2 litres. The air left in lungs is useful in uninterrupted gaseous exchange.
• Inspiratory reserve volume ( I.R.V = complemental air) : Volume of air in excess of tidal volume which can be inhaled due to forceful inspiration.
• Expiratory reserve volume ( E.R.V = Supplemental air): Volume of air in excess of tidal volume which can be exhaled due to forceful expiration 1 – 1.1 litres.
• Vital capacity (v.C): It is the total volume of air inspired and expired to a maximum level. It is the sum total of tidal volume, inspiratory reserve volume and expiratory reserve volume
VC = T.V. + I.R.V. + E.R.V.
It is 3.5 to 4.5 litres
i) The vital capacity is higher in athletes mountaineers or mountain – dwellers and lower in non-athletes, people living in plains, women, old individuals, cigarette smoker.
ii) Higher the vital capacity, higher is the amount of air exchanged in each breath.
• Inspiratory capacity (IC): It is the total volume of air that can be inhaled after normal expiration. It includes tidal volume and inspiratory reserve volume.
IC = T.V. + I.R.V
It is 2.5 to 3.0 litres
• Expiratory capacity (E.C.): It is the total volume of air that can be exhaled after normal inspiration. It includes tidal volume and expiratory reserve volume.
EC = T.V. + E.R.V
Its value is 1.5 to 1.6 litres
• Functional residual capacity (FRC); It is the sum total o residual volume and the expiratory reserve volume.
F.R.C. = R.V. + E.R.V.
Its value is 2.3 to 2.7 litre
• Total lung capacity (TLC): It is the total amount of air present in the lungs and the respiratory passage after maximum inspiration. It is the sum total of vital capacity and residual volume
TLC = VC + RV or TLC = TV +IRY + ERV + RV
Its value is 5 to 6 litre
• Alveolar ventilation: It is the rate at which the fresh air reaches the alveoli and adjoining areas like alveolar ducts, alveolar sacs and respiratory bronchioles. It is calculated as.
• Alveolar ventilation per minute
= Rate of respiration × (TV – dead space volume)
= 12 × ( 500 -150 )
= 12 × 350
= 4.2 litres / minute
EXCHANGE OF GASES
• Alveolar air is separated from blood present in surrounding blood capillaries by very thin partition of 0.2 μm thickness. It is called respiratory membrane. The membrane consists of alveolar surfactant, alveolar epithelium, epithelial basement membrane, a thin interstitial space, capillary basement membrane and capillary endothelial membrane.
• Diffusing capacity of a gas across a membrane is the volume of gas that diffuses per minute for a pressure difference of 1mmHg. The rate of diffusion of CO2 is 20 times faster than that of oxygen while oxygen diffuses faster ( twice) than nitrogen. Partial pressure of O2 in alveolar air (PO2) is about 100-104 mmHg while that of deoxygenated blood in alveolar capillary is 40mmHg. Therefore, oxygen diffuses into blood and combines with haemoglobin to form oxyhaemoglobin. Pressure of (PO2) oxygenated blood is 95 mmHg. PCO2 ( pressure of carbon dioxide) of alveolar capillary blood is 46 mmHg, while in fresh alveolar air it is 40mmHg. As the diffusing capacity of CO2 is 20 times higher than that of O2, CO2 of blood rapidly passes out into alveolar air. Its partial pressure in oxygenated blood is 40 mmHg.
• Gaseous exchange occurs again in the tissues cells and capillary blood through the interstitial fluid. Partial pressure of oxygen, PO2 in respiring cells is 20mmHg, tissue fluid is 40mmHg, while it is 95mmHg in capillary blood. Therefore, O2 diffuses from blood into tissue fluid and from there into cells. Blood leaving the tissue capillaries has PO2 of about 40mmHg. PCO2 of blood capillaries is 40mmHg, tissue fluid 45mmHg and that of cells 52mmHG. Therefore, carbon dioxide diffuses out of cells into tissue fluid and form tissue fluid into blood. Blood leaving the tissue capillaries has a PCO2 of 46mmHg.
TRANSPORT OF OXYGEN
• Oxygen is carried by blood in two forms in solution and as oxyhaemoglobin as RBCs
1. IN SOLUTION
- Oxygen is soluble in plasma to a small extents under normal conditions of temperature and pressure. Hence most of it is carried by red blood cells. About 3% of oxygen is transported by blood in dissolved form in plasma of blood. Example, out of about 4.6ml of oxygen entering each 100ml of blood in lungs only 0.17 ml travels in solution form in the plasma.
2. AS OXYHAEMOGLOBIN
- RBC contain a protein called haemoglobin. It has four polypeptide chains and four haem groups attached to it or 4 atom of iron in ferrous form (Fe2+), thus it can react with 4 molecules of oxygen to form Hb4O8. This is called oxyhaemoglobin. This combination process is called oxygenation.
- On an average 15gm of haemoglobin (Hb) is present in 100ml of blood. 1gm of Hb combines with 1.34ml of O2. Thus 100ml of blood carries approximately 20ml of O2 (19.4 ml to be exact)
- But when blood reaches the tissues, its O2 concentration reduces gradually to 14.4 ml which is collected by veinules and vein. Thus 5ml of O2 is transported by 100ml of blood under normal condition.
- Haemoglobin has higher affinity for oxygen and this affinity is increased by fall in PCO2 of blood.
- At the alveoli, venous blood has low oxygen and is exposed to low PCO2 of alveolus, thus oxygen diffuses into red blood cells and form oxyhaemoglobin ( bright red). As CO2 diffuses from blood to alveolus, blood PCO2 falls increasing further uptake of oxygen.
- Oxyhaemoglobin remains unchanged till it reaches the tissues where it dissociates readily to release oxygen.
OXYGEN – HAEMOGLOBIN DISSOCIATION CURVE ( OXYGEN DISSOCIATION CURVE)
• The percentage of haemoglobin that is bound with O2 is called percentage saturation of haemoglobin.
• The relationship between the partial pressure of oxygen (PO2) and percentage of saturation of the haemoglobin with oxygen (O2) is graphically illustrated by a curve called oxygen haemoglobin dissociation curve.
• Under normal conditions, the oxygen haemoglobin dissociation curve is sigmoid shaped or ‘S’ shaped. The lower part of the curve indicates dissociation of oxygen from haemoglobin. The upper part of the curve indicates the acceptance of oxygen by haemoglobin. When the partial pressure of oxygen is 255mmHg the haemoglobin gets saturated to about 50%. It means blood contains 50% oxygen. The partial pressure at which the haemoglobin saturation is 50% is called P50. At 40mmHg of partial pressure of oxygen the saturation is 75%. It becomes 95% when the partial pressure of oxygen is 100mmHg.
• Haemoglobin does not take up oxygen are low PO2, but as oxygenation of pigment occurs, its affinity for more O2 increases. In haemoglobin where 4 sub-units are present, acquisition of one molecule of oxygen increases the affinity of neighbouring haems for oxygen. This is known as co-operativity between active sites.
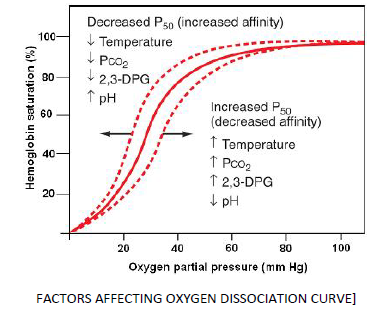
i) Temperature: At higher temperature haemoglobin gives up oxygen more readily and dissociation curve shits to the right. This is of physiological importance because increased temperature means higher metabolic rate or higher oxygen requirement.
ii) pH: Increase in CO2 or other acids lower the pH of plasma and shifts the dissociation curve to the right. At higher CO2 concentration more O2 is given up at any oxygen pressure.
iii) PCO2: CO2 lowers the oxygen affinity of haemoglobin even if the pH is kept constant. Oxygen dissociation curve shifts to the right and release more O2 with increase in PCO2
iv) 2,3-diphosphoglyceric acid ( 2,3-DPG) : It is present in the red blood cells of adult, formed from 3-phosphoglyceric acid. It competes for oxygen binding sites in haemoglobin molecule. As it binds to the β- chain of HbA, it causes right shift of dissociation curve resulting in higher P50.
v) Lower CO2 concentration, lower body temperature lower 2,3-DPG lower the P50 and the curve moves to the left.
BOHR EFFECT
• Shifting of the oxygen haemoglobin dissociation curve to the right by increasing carbon dioxide partial pressure is known as Bohr effect. It is named after Danish physiologist Christian Bohr.
• The presence of carbon dioxide decreases the affinity of haemoglobin for oxygen and increases release of oxygen to the tissues.
• The pH of the blood falls as its CO2 content increases so that when PCO2 rises the curve to the right and P50 rises.
• In the tissue, PO2 is between 10 to 40 mmHg and PCO2 is high around 45mmHg. So, an active tissue will have high PCO2, low pH and raised temperature leading to the dissociation of oxygen. Oxygenated blood passing through inactive cells does not given up oxygen even if its PCO2 is low but active cells readily gives oxygen as PCO2 is very high.
TRANSPORT OF CARBON DIOXIDE
I. IN DISSOLVED STATE
Because of its high solubility, about 7% carbon dioxide gets dissolved in the blood plasma and is carried in solution to lungs. Deoxygenated (venous) blood and oxygenated (arterial) blood carry about 2.7ml and 2.4ml of CO2 per 100ml of blood in dissolved state in plasma respectively.
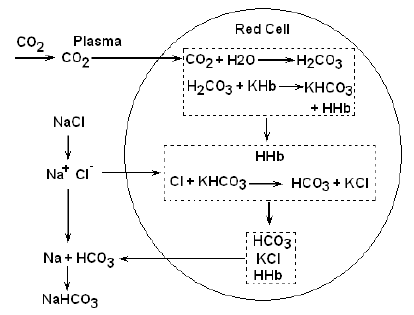
II. IN THE FORM OF BICARBONATE
- The dissolved carbon dioxide in the blood reacts with water to form carbonic acid. This reaction is very slow in the blood plasma, but occurs very rapidly inside RBCs because a zinc containing enzyme, the carbonic anhydrase, present in RBCs,
accelerates its rate about 5000 times.
- Due to this, about, 70% of CO2, received by blood from the tissues, enters the RBCs where it reacts with water to form carbonic acid (H2CO3).
- Carbonic anhydrase is exclusively found in R.B.Cs. All other tissue contains it in traces except stomach and pancreas in which have considerable amount. This enzyme not only speeds up the formation of carbonic acid (H2CO3) but also rapidly converts it back to carbon dioxide and water when blood reaches the lungs.
- Almost as rapidly as formed all carbonic acid of RBCs dissociates into hydrogen (H+) and bicarbonate ions (HCO3 - ).
- The most of bicarbonate ions (HCO3- ) formed with RBCs diffuse out into blood plasma along the concentration gradient.
- When the whole blood is saturated with carbon dioxide, the following changes are seen.
(i) The bicarbonate content of plasma and corpuscles increase.
(ii) The chloride content of plasma is diminished and that of the cells is increased.
(iii) The total base (cations) of both plasma and corpuscles remain unchanged.
(iv) The water content and the volume of corpuscles increase.
- When carbon dioxide is removed from a sample of blood, reverse changes take place. From these observations, it is evident that, when carbon dioxide enters blood, chlorine from plasma enters the RBCs, while the base (NA) is left behind.When carbon dioxide escapes the plasma and combines with the base (Na) again. Due to this alternate movement of chlorine ions, this phenomenon is called chlorine shift or Hamburger phenomenon.
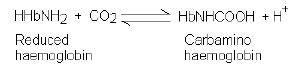
III. AS CARBAMINOHAEMOGLOBIN
- In addition to reacting with water, carbon dioxide also reacts directly with amine radicals (NH2) of haemoglobin to form an unstable compound carbaminohaemoglobin. This is a reversible reaction.
- A small amount of carbon dioxide also reacts in this same way with the plasma proteins. About 23% CO2 is transported in combination with haemoglobin and plasma proteins
HAEMOGLOBIN AS BUFFER
• Addition of hydrogen ions would make the blood acidic. However, most of the hydrogen ions are neutralized by combination with haemoglobin, which is negatively charged, forming acid haemoglobin. This reduces the acidity of the blood and also releases additional oxygen.
• If the blood becomes too basic, acid haemoglobin dissociates, releasing hydrogen ions.
HHb→ H+ + Hb
Thus, the haemoglobin also acts as buffer, a substance that keeps the pH from fluctuating. The haemoglobin of the foetus has a higher affinity for oxygen than the mother’s haemoglobin. After birth, the foetal haemoglobin is gradually replaced by adult haemoglobin.
RESPIRATORY PIGMENTS AND ANIMALS CONTAINING IT
1. Haeocyanin
A copper containing blue pigment occur in plasma of crustaceans, snails and cephalopods.
2. Chlorocruorin
It is an iron containing green pigment, occur in plasma of annelids polychaete.
3. Pinnaglobin
It is a manganese containing brown pigment occurs in blood fluid of some mollusks (pinna).
4. Echinochrome
Contains iron and occur in the coelomic fluid of sea urchin (echinoderm)
5. Vanadium
Contains vanadium. Present in the blood of tunicates ( urochordates). Ciona contains vanadium in plasma and Ascidia contains in green blood corpuscles (vanadocytes)
6. Myoglobin
Haemoglobin of the muscle
7. Molpadin
Occur in molpadia ( echinodermata)
RESPIRATORY CENTRE
• It controls the rate of respiration. Respiratory centre is located in medulla oblongata and pons. It has the following well dispersed components.
i) Dorsal Respiratory Group
Located dorsally along length of medulla with neurons interconnected to sensory termination of glossopharyngeal ( sensory signals from preripheral chemoreceptors) and vagus (sensory signals from lungs and stretch receptors of bronchi) nerves. The area is connected through nerves to phrenic muscles of diaphragm. Nervous signals from this group brings about normal resting inspiration. Expiration occurs through elastic recoil of thoracic wall and lungs
ii) Pneumotaxic Area
It occurs in pons and is meant for switching off normal inspiration when the limit of lung filling is reached. The latter is however also dependent upon the strength of signal 0.5sec when signal is strong and 5 sec when signal is poor.
iii) Ventral Respiratory Group
It occurs ventrolaterally anterior to dorsal respiratory group. The group has two types of neurons, inspiratory and expiratory. They are normally inactive but when the respiratory drive is greater than normal, the group is activated. It results in deeper and quicker inspiration and expiration.
iv) Chemosensitive Area
It lies in the medulla near the place of entry of glassopharyngeal and vagus nerves. It is sensitive to blood carbon dioxide and hydrogen ion concentration. Chemosensitive areas are connected to other areas of respiratory centre.
RESPIRATORY DISORDERS
1. TUBERCULOSIS
Bacterial disease caused by Mycobacterium tuberculosis. Infection of several parts but common of lungs. Vaccination with B.C.G. ( Bacillus – Calmette – Guerin)
2. PLEURISY ( Pleuritis)
Inflammation of pleura or accumulation of pleural fluid. Presence of excess fluid in the pleural cavity is called hydrothorax. Presence of air in pleural space is called pneumothorax.
3. EMPHYSEMA
It is a permanent abnormal pathological inflation of air spaces distal to terminal bronchioles due to destruction of pulmonary tissues especially alveolar septa and flattening of alveolar ducts. There is little alveolar elasticity. Lung size increases but ventilation is poor.
Emphysema develops due to infection, smoking and chronic bronchitis. The disease cannot be cured completely because it involves irreversible change in the alveoli. Bronchodilators, antibiotics and O2 therapy are used to provide relief and retard progression of disease.
Emphysema is preventable if care is taken to reduce exposure to smoke and air pollutants.
4. ASPHIXIA
Paralysis of respiratory centre due to excessive carbon dioxide commonly due to irreversible combination of carbon monoxide with haemoglobin to form carboxyhaemoglobin. It results in death. Common in closed rooms with coal burning, kerosene lamp.
5. PNEUMONIA
- It is a disease of lungs with an incubation period of 1-3 days and characterized by accumulation of mucus/ fluid with dead WBCs in alveoli and bronchioles so that breathing becomes difficult. It is of several types. Common pneumonia is caused by gram(+) nonmetal paired bacterium called Streptococcus or Diplococcus pneumonia. Other bacterium, fungi, virus, mycoplasma and even some protozoans also produce the disease.
- Three types of individual are more susceptible to disease; elders, infants, immune-compromised. The disease is of two types – bronchopneumonia ( young children, elderly person) and lobar pneumonia ( 10-50 years)
- The disease is transmitted through droplets. There is sudden chill, chest pain, cough with rusty mucoid sputum, rise in temperature, rapid shallow breathing and reduced oxygen level of blood due to poor gaseous exchange. Abdominal distension is also common. Useful drugs are erythromycin, tetracycline, sulphonamide. Bronchiodilator drugs provide some relief untreated pneumonia leads to death.
6. HYPOXIA ( Anoxia)
Shortage of oxygen supply to the body due to:
a) Normal shortage in air as on high mountain.
b) Anaemia.
c) Histotoxicity or poisoning of electron transport system.
7. HICCOUGH ( Hiccup)
Inspiratory spasm caused by sudden contraction of diaphragm accompanied by loud closure of glottis.
8. COUGH
Violent expiration for expulsion of mucus and particles.
9. WHOOPING COUGH ( Pertussis)
Cough with inspiratory whoop caused by Bordetella (Haemophilus) pertussis.
10. BRONCHIAL ASTHMA
Due to narrowing of bronchi and spams in bronchial muscles. The disorder is generally due to hypersensitivity of bronchioles to foreign substances. There is intense coughing and difficulty in exhalation. Mucous glands becomes over active producing a lot of mucus that clogs bronchioles and bronchi. Exposure to allergens should be avoided. Bronchodilators, inhalers and antibiotics are given for relief and protection against infection.
11. HAY FEVER
It is an allergic disorder of nasal lining. It develops due to hypersensitivity of the lining to pollen grains or any other foreign particles.
12. ATELECTASIS
It is an inability of lungs to expand at birth. This is mainly due to deficiency of surfactants.
13. SILICOSIS
It is due to long exposure to dust containing silicon compounds. Workers of glass industry, potters, gold and copper miners develop progressive fibrosis in the liver.
14. ASBETOSIS
It is due to inhalation of asbestos – fibres, which may result in cancer of pleura.
15. DIPHTHERIA
Infection of bacterium, corynebacterium diphtheria of upper respiratory tract that produces pseudomembrane in throat. Pseudomembrane obstructs breathing causing hypoxia.
16. BRONCHITIS
Inflammation of bronchi and bronchioles due to hypertrophy and hyperplasia and seromucous gland and goblet cells. There is a regular coughing with thick greenish yellow sputum indicating infection and excessive secretion of mucus. It is commonly caused by viral infection of nasal tract followed by bacterial infection. The disorder is common in smokers and persons exposed to CO rich polluted air. Persons suffering from bronchitis should avoid smoke, irritating chemicals and pollutants. Bronchodilators provide
symptomatic relief. Antibiotics are used to cure infection.
17. CYANOSIS
Bluish colouration of skin and mucous membranes due to reduced haemoglobin in blood.
18. EPISTAXIS
Nose bleed. Quite common due to any scratching of nasal membranes. Nasal membrane is highly vascular. Epistaxis can also occur due to hypertension.
19. PHARYNGITIS
Inflammation of Pharynx
20. LARYNGITIS
Inflammation of larynx.
21. SNEEZING
An involuntary, sudden, violent and audible expulsion of air through mouth and nose.
22. YAWNING
A deep involuntary inspiration with mouth open, often accompanied by act of stretching.
23. SARS
It is a killer atypical pneumonia called severe acute respiratory syndrome. The disease is caused by variant of common cold corona virus which spreads by droplet and other methods. There is an initial fever (100.4OF), headache, body aches, dry cough and then difficult breathing.
24. OCCUPATIONAL LUNG DISEASES
i) Black lung: Affects coal workers
ii) Chronic Beryllium disease (CBD): It affects workers in a variety of metallurgical occupations.
iii) Byssinosis brown lung disease: It often affects cotton and textile workers when bacteriua released from cotton or other material are inhaled and grow in lungs.
iv) Occupational asthma: It can affect people who work with variety of materials, like dyes, resins, leather, latex, rubber, etc.
• It is always advisable to undertake preventive measures in work place involving pollution risk by:
(i) Reducing emission of harmful dust and chemicals
(ii) Using protective gear and clothing.
(iii) Short duties.
(iv) Informing workers about risks and preventive measures.
(v) Regular health check up.
MOUTH SICKNESS
• It is hypoxial or oxygen shortage syndrome, which occurs at altitude of 3500 meters and above. There is decrease in atmospheric pressure as well as oxygen content of atmosphere. Reduced atmospheric pressure, reduces the amount of air taken into the lungs during inspiration. Reduced oxygen contents reduces its partial pressure and rate of diffusion into the blood. Hypoxia increases. As a result, body obtains less O2 and therefore, produces lesser energy. However, requirement of energy at high altitude is higher due to low temperature and increased physical strain. Effects of deficient availability of energy begins to appear within 8-24 hours.
• It is characterized by breathlessness, fast breathing, nausea, vomiting, cyanosis, headache, muscular weakness and mental fatigue. After sometimes, the symptoms subside due to increased concentration of 2,3-diphosphoglycerate in erythrocytes that attracts more oxygen to form HbO2 even PO2 is lower. Soon rise in haemoglobin and erythrocytes count shall start.
TERMS RELATED TO BREATHING
(i) Euponea: Normal breathing
(ii) Hypoponea: Slower breathing
(iii) Hyperponea: Rapid breathing
(iv) Apnoea: No breathing
(v) Dyspnoea : Painful breathing
(vi) Orthopnoea: Difficult breathing in horizontal position.
(vii) Tachypnoea: Rapid shallow breathing.
(viii) Polypnoea: Rapid deep breathing
(ix) Hypercapnia: Excess of CO2 in blood.
(x) Hypocapnia: Low CO2 concentration in blood.