
Download the latest CBSE Class 12 Physical Education Children And Women In Sports Notes Set 01 in PDF format. These Class 12 Physical Education revision notes are carefully designed by expert teachers to align with the 2026-27 syllabus. These notes are great daily learning and last minute exam preparation and they simplify complex topics and highlight important definitions for Class 12 students.
Revision Notes for Class 12 Physical Education Children And Women In Sports
To secure a higher rank, students should use these Class 12 Physical Education Children And Women In Sports notes for quick learning of important concepts. These exam-oriented summaries focus on difficult topics and high-weightage sections helpful in school tests and final examinations.
Children And Women In Sports Revision Notes for Class 12 Physical Education

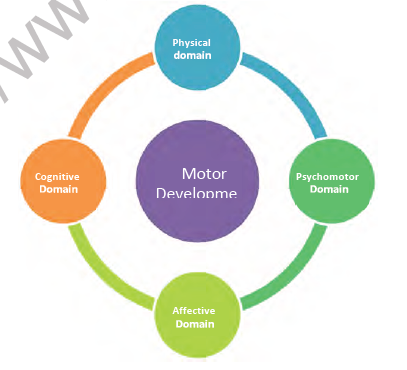

Gross and Fine Motor Skills
On the basis of muscular development, Motor development can be divided into two major areas: gross motor skills and fine motor skills.
Gross motor skills include activities that involve moving major areas of the body. Activities like running, jumping, climbing, throwing, standing, and sitting are examples of gross motor skills.
Fine motor skills require more precision and involve hand and eye coordination. These skills, which seem simple to adults, require concentration for children to develop them. A snooker shot is an example of fine motor skill.
Extension Activity
Working in pairs, list the following activities into Gross and Fine Motor Skills.
• Climbing up, down, over, under and through things
• Completing shape puzzles
• Cutting shapes with scissors
• Dumping and filling a bucket
• Jumping
• Making shapes with play dough
• Running
• Stacking blocks
• Stringing beads
• Throwing and catching
Open and Closed Motor Skills
Sports skills can be classified according to how much they are affected by the sporting environment. Environmental stimuli include
Other people – for example, a netballer reacting to their own and the other team's players
Terrain/surface – for example, a cross-country runner running on muddy and dry ground
Weather – for example, a golfer playing on a windy day
Situation – for example, the venue and crowd Performers need to have a good perception of these stimuli to adapt their skills to best suit the environment. These skills may be divided into Open and Closed Skills.
Open skills: An open motor skill is a skill performed in an unstable environment, where the start point is determined by the environment. Team-based sports such as Netball, Football, and Hockey involve open skills where the environment is continually changing, and so movements have to be continually adapted.
Closed skills: A closed motor skill is a skill which is performed in a stationary environment, where the performer chooses when to start the skill. These skills take place in a stable, nonhttps team based, predictable environment, and the performer knows what to do and when. For example, a free throw in Basketball and serving in Squash or Tennis.
Locomotor and Manipulative Skills
Fundamental movement skills provide a foundation for many physical activities including play, games, outdoor recreation and sports. Having these skills is an essential part of enjoyable participation and a lifelong interest in an active lifestyle. Fundamental movement skills include stability, locomotive, and manipulative or object control and skills.
Stability skills involve the body balancing either in one place (static) or while in motion (dynamic). Stability skills in this resource include landing, balance (static and dynamic) and rotation.
Locomotor Skills involve the body moving in any direction from one point to another.
Locomotor skills include walking, running, dodging, jumping, hopping and skipping.
Manipulative skills involve handling and controlling objects with the hand, the foot or an implement (stick, bat or racquet). Manipulative skills in this resource include throwing and catching, striking with the hands, feet and an implement (e.g. kicking, volleying, batting and dribbling).
Discrete, Serial and Continuous Motor Skills
The Temporal Aspect refers to the organisation of the motor skill in time, Discrete skills are brief, well-defined actions that have a clear beginning and end. They are single, specific skills, which make up the actions involved in a variety of sports such as hitting and throwing. For example, a penalty flick in Hockey.
Serial Skills are a group of discrete skills strung together to make a new and complex movement. For example, the sequence of skills for the triple jump.
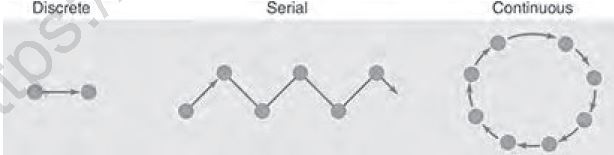
Continuous skills have no obvious beginning or end. The end of one cycle of movements is the beginning of the next, and theskill is repeated like a cycle. These skills could be stopped at any moment during the performance of the skill. For example, Swimming, Running, Cycling.
Factors that Affect Motor Development
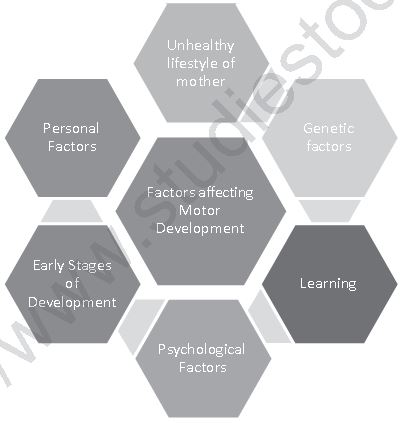
Human beings are different from others in terms of personality, appearance, motor movements etc. As a result, the rate and level of motor development also varies. Therefore, to understand the stages of Motor development it is essential we discuss factors that affect it. The primary factors affecting Motor development are individual ability, environment and the given task.
Do you know
Developmental milestones are behaviours or physical skills seen in infants and children as they grow and develop. Rolling over, crawling, walking, and talking are all considered milestones. The milestones are different for each age range. There is a normal range in which a child may reach each milestone.
Delayed milestones, also called developmental delays, describes the condition where a child does not reach one of these stages at the expected age.
Let us study factors affecting Motor development in detail.
1. Lifestyle of mother: An individual’s growth and development journey starts in the mother’s womb as a zygote. For the next nine months of foetal period the zygote develops extremities, teeth, nose, eyes, ears, central nerve system etc. During this period the baby is totally dependent on the mother. As a result, the mother lifestyle affects the baby. An unhealthy lifestyle like imbibing certain medicines, drugs, smoking, alcohol and other unhealthy food leads to growth deficiency, CNS dysfunctions, other anomalies and complications. Maternal nutrition should be balanced and must include all nutrients like protein, calcium, iron-rich foods, vitamins, and extra calories as per requirement of the body.
2. Genetic factors: Abnormal development can be caused by gene-based disorders or chromosomal disorders. Deformities like heart defects, respiratory distress syndrome, Musculo-skeletal deformities etc. and Down Syndrome, which includes short stature, late or no speech development, slow development of fine motor skills etc. may happen due to genetic factors.
3. Learning: Learning is one of the important factors that affect growth and development. Learning requires readiness to seek or acquire new information or skills.
A child must be physiologically ready to develop strength, endurance and flexibility that will help to control the body, and psychologically ready to acquire skills. In other words, the child must be physically and mentally ready to seek information.
Motivation and timely reinforcement promote learning. Individual differences including race, gender, culture and socioeconomic status may affect growth and development process.
4. Psychological Factors: Self-esteem plays an important role in growth and development of the individual. An individual with high self-esteem in the physical arena is not likely to give up physical activity. It motivates her/him to join and sustain the particular activity. Other factors including self-confidence, self-worth, self-image, emotions, also play a vital role in growth and development.
5. Early Stages: Portents and teaches should work on a programme where stimulation and deprivation are given systematically. While the more stimulation and opportunities a child is provided in order to develop both gross and fine motor skills, the faster her/his capacity increases. For instance, if a child is encouraged to play outside on park equipment or other areas where she/he can climb, run, and play, her/his gross motor skills will develop quickly. Additionally, fine motor skills develop when children are encouraged to play with their hands, hold and touch smaller items, feed themselves, and draw or colour. Timely immunization also helps to prevent disease from child and would not hinder learning process. However, we must keep in mind the child’s readiness to learn. Now-a-days parents provide stimulation too early like focus on swimming, reading, writing etc in early stages. This may have an adverse effect on the child’s growth and development.
6. Personal Factors: Physical characteristics, intelligence, aptitude, height, weight, age, muscle fibres, length of fibres, bone structure, gender, diseases are factors that affect motor development. Taking a balanced diet or proper proportion of nutrition in food is required to promote motor development. Malnutrition leads to disease, low immunity, and adversely affects the child’s health and motor development. Starvation, overeating, eating disorders negatively affect motor development leading to obesity, diabetes, heart disease etc. Good fitness level leads to good health, better reflexes and readiness of muscles to do complex movements. To keep body fit, children should be exposed to outdoor activities also. These activities should be planned in such way that there is focus on muscular aspect of movement for gross and fine motor skills development.
I. Tick the correct options
1. An activity that is NOT an example of gross motor skills is
(a) drawing
(b) standing
(c) throwing a ball
(d) jumping
2. An activity that is NOT an example of fine motor skills is
(a) using cutlery
(b) riding a bike
(c) building a toy tower
(d) cutting shapes using scissors
II. Answer the following questions briefly
1. Define Motor Development.
2. Briefly describe the domains of motor development.
3. Describe any one factor that affects motor development.
4. List down the major factors affecting motor development.
III. Answer the following questions in 150-200 words
1. Explain factors affecting motor development.
Physical Activity Guidelines at Different Stages of Growth and Development
World Health Organisation (WHO) has identified lack of physical activity, or physical inactivity, as the fourth leading risk factor for global mortality (6% of deaths globally).
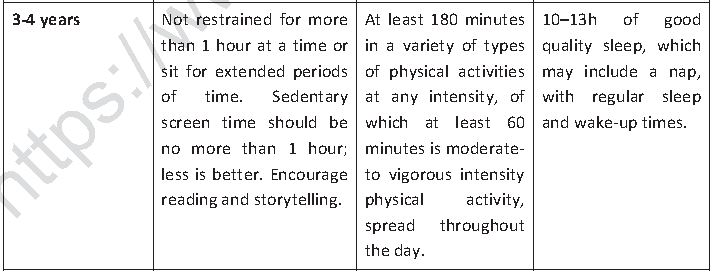
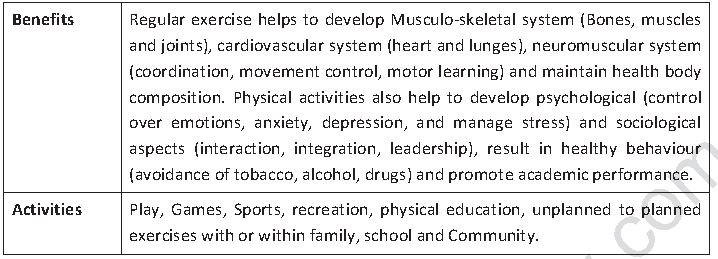
Regular participation in physical activities and sports provides ample opportunities to maintain physical, mental and social health. Participation in sports and physical activity results in benefits like an increase in self-confidence and self-esteem, a better control over emotions, reduction in levels of stress, anxiety and depression, maintenance of healthy weight social interaction and achieving high performance in academics. Regular physical activities help in not just physical, but also social, emotional and mental growth and development of infants, children, adolescents and adults. Physical activities should be encouraged among children to ensure strong muscles and bones. Children and young people should not be allowed to sit for long hours watching TV, playing computer games and travelling by car.
WHO has developed certain guidelines – Global Recommendations on Physical Activity for Health – with the overall aim of providing national and regional level policy makers with guidance on the frequency, duration, intensity, type and total amount of physical activity needed for the prevention of Non-Communicable Diseases or Lifestyle Diseases.
Children Under 5 Years of Age
“Achieving health for all means doing what is best for health right from the beginning of people’s lives,” says WHO Director-General Dr Tedros Adhanom Ghebreyesus. “Early childhood is a period of rapid development and a time when family lifestyle patterns can be adapted to boost health gains.” Children under five must spend less time sitting watching screens, or restrained in prams and seats, get better quality sleep and have more time for active play if they are to grow up healthy.
The following guidelines are recommended for healthy children aged Under 5 years, irrespective of gender, race, ethnicity, cultural background, and the socio-economic status of the family.
These are also relevant for children with different abilities. Children with a medical condition or disability should consult with health professionals before undertaking these activities. The goals of these guidelines are to recommend time spent on physical activities, and on sleep and sedentary activities to get health benefits. The age group further divided in to three group namely Less than 1 year, 1 to 2 years, 3 to 4 years.
Infants (Less than 1 year)
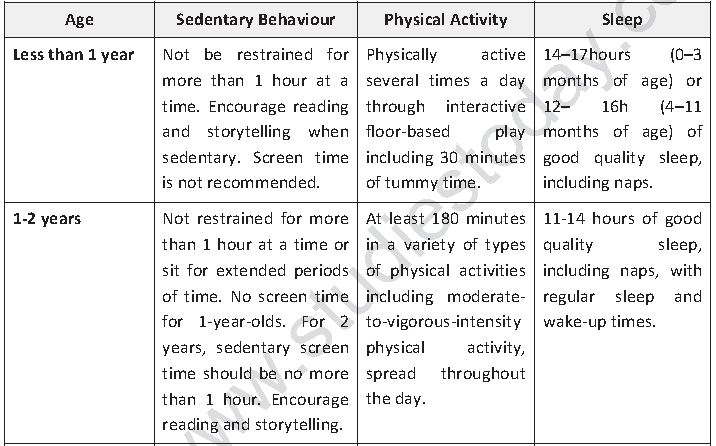
Infants should be provided enough space and open environment to promote movement and minimize restrictive or sedentary behaviour so that they may explore their surroundings.
Babies should be encouraged to be active throughout the day, every day. Before your baby begins to crawl, encourage her/him to be physically active by reaching and grasping, pulling and pushing, moving her/his head, body and limbs during daily routines, and during supervised floor play. This includes giving the baby 30 minutes in prone position (tummy time). Playing equipment should not be too small that can be swallowed or having sharp edges or prepared with toxic material. Activities like crawling and rolling should be performed on mat or sheet size of at least 7 feet by 4 feet. Once babies can move around, encourage them to be as active as possible in a safe, supervised and nurturing play environment. During sedentary timing child must be engaged in reading and storytelling for encouragement. For 0-3 months ages 14-17 hours and for 4-11 months of age baby should have good quality sleep that includes naps.
Toddlers (1-2 years of age)
During this period, the child should not be involved in any sedentary activity which is more than one-hour long including being restrained in prams/strollers, high chairs, or strapped on a caregiver’s back, or sitting for extended periods of time. Once they learn to sit and stand toddlers should be encouraged to undertake fundamental physical activity like walking, running, jumping, catching, throwing, leaping etc. In this group sedentary screen time like involvement with computer games, watching TV or video is not recommended. Engagement in reading and storytelling should not be more than one hour. It is recommended toddlers get 11-14 hours of good quality sleep, including naps, with regular sleep and wake-up times.
Children 3–4 years
Children should spend at least 180 minutes in a variety of types of physical activities at any intensity, of which at least one hour is spent in moderate to vigorous intensity physical activity. This should be spread throughout the da y, indoors or outside. In the 180 minutes of physical activity, we can include light activity such as standing up, moving around, rolling and playing, as well as more energetic activities like skipping, hopping, running and jumping.
Active play, such as using a climbing frame, riding a bike, playing in water, chasing games and ball games, is the best way for this age group to get moving. Sedentary time should not be more than one hour, and during this period engagement in reading and storytelling should be encouraged. Quality sleep between 10-13 hours is recommended which includes a nap, with regular sleep and wake-up times.
All these recommendations are divided into three components Physical activity, sedentary behaviour and sleep. Lesser sedentary time and more moderate to vigorous intensity physical activity with sufficient sleep can provide additional health benefits.
Children and Youth 5-17 Years
These recommendations are relevant to healthy children and youth between 5 to 17 of age irrespective of gender, race, ethnicity or socio-economic status.
Children and youth with a specific medical condition or disability may follow these recommendations under advice of a medical official or with the help of the school special education teacher. Activities should be done in a progressive manner, for example starting the session with simple exercises to complex, gradually increasing the frequency, duration and intensity of the activities. There are various stages of growth in this age group, wherein at every stage the type of activities changes. The chief aim of activities during this age group is to improve cardiorespiratory and muscular fitness, bone health, cardiovascular and metabolic health biomarkers and to reduce symptoms of anxiety and depression.

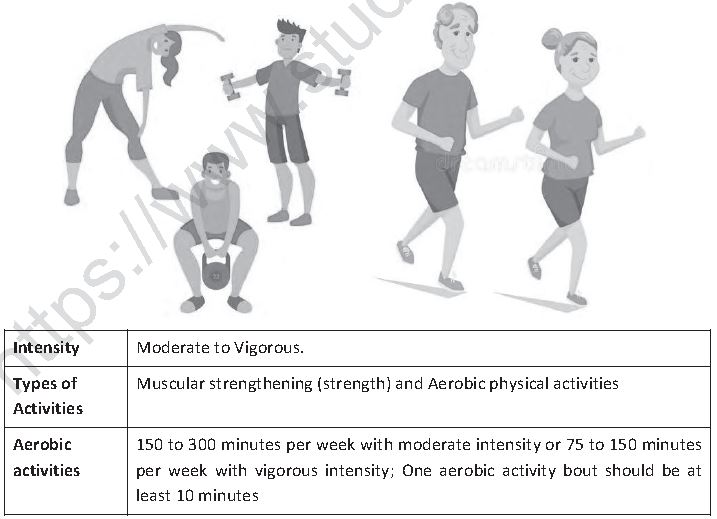
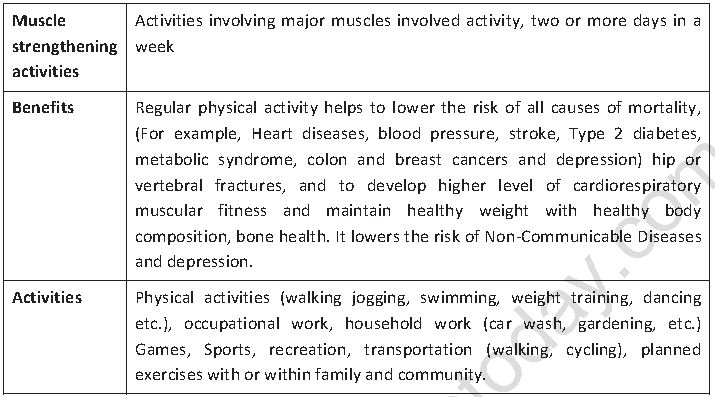
Adults 18-64 Years
These recommendations are relevant to healthy adults aged between 18 to 64 irrespective of gender, race, ethnicity or social-economic status. Adults youth with disabilities may follow these recommendations with adjustment as per capacity or limitations. Adult having any medical condition should follow the advice of medical official. Activities should be done in progressive manner for example to start session with simple exercises to complex, gradually increase frequency, duration, intensity of the activities.
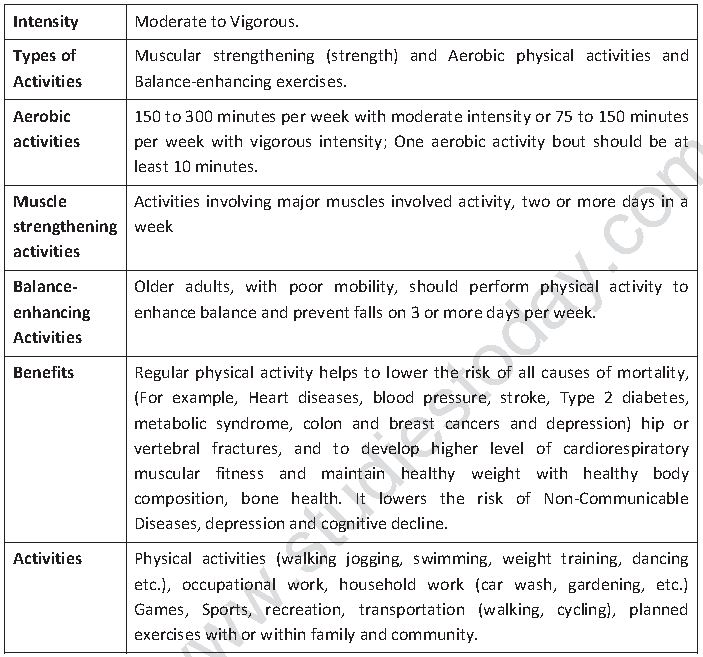
Older Adults 65 Years and Above
These recommendations are relevant to healthy older adults aged between 65 and above irrespective of gender, race, ethnicity or social-economic status. These recommendations are also relevant for individuals suffering from chronic NCD conditions Adults, youth with disabilities may follow these recommendations with adjustment as per capacity or limitations. Individuals with specific health conditions, such as cardiovascular disease and diabetes, may need to take extra precautions and seek medical advice before trying to achieve the recommended levels of physical activity for older adults. Activities should be done in progressive manner for example to start session with simple exercises to complex, gradually increasing frequency, duration and intensity of the activities as per their ability and as conditions allow.
Do you Know?
Type of physical activity: includes aerobic, strength, flexibility, balance.
Duration: is the length of time in which an activity or exercise is performed. Duration is generally expressed in minutes.
Frequency: is the number of times an exercise or activity is performed. Frequency is generally expressed in sessions, episodes, or bouts per week.
Intensity: refers to the rate at which the activity is being performed or the magnitude of the effort required to perform an activity or exercise.
Volume: Aerobic exercise exposures can be characterized by an interaction between bout intensity, frequency, duration, and longevity of the programme. The product of these characteristics can be thought of as volume.
Moderate-intensity physical activity: On an absolute scale, moderate intensity refers to activity that is performed at 3.0–5.9 times the intensity of rest. On a scale relative to an individual’s personal capacity, moderate-intensity physical activity is usually a 5 or 6 on a scale of 0–10.
Vigorous-intensity physical activity: On an absolute scale, vigorous intensity refers to activity that is performed at 6.0 or more times the intensity of rest for adults and typically 7.0 or more times for children and youth. On a scale relative to an individual’s personal capacity, vigorous intensity physical activity is usually a 7 or 8 on a scale of 0–10.
Aerobic activity: also called endurance activity, improves cardiorespiratory fitness.
Examples of aerobic activity include: brisk walking, running, bicycling, jumping rope, and swimming.
Sedentary behaviour: is characterized by a very low energy expenditure, such as sitting, reclining or lying down
Sleep behaviour: Duration and timing of sleep. For children under 5 years of age includes both at night and daytime naps. Toddler Child aged 1 to under 3 years (12.0–35.9 months).
Tummy time: Time an infant spends lying on her/his stomach (in prone position) while awake with unrestricted movement of limbs.
Nap: Period of sleep, usually during the daytime in addition to usual night time sleep.
I. Tick the correct options
1. Minimum duration of activity should be _ per week at vigorous intensity in adults above 65 years of age.
(a) 75 minutes
(b) 150 minutes
(c) 300 minutes
(d) 450 minutes
2. Rate at which the activity is being performed is known as _
(a) Volume
(b) Intensity
(c) Type of Activity
(d) Frequency
II. Answer the following questions briefly
1. Write down Physical activities exercise guideline for under 5 of age.
2. Briefly tell about physical activities exercises guideline for above 65 of age.
III. Answer the following questions in 150-200 words
1. Describe Physical activities exercise guideline for all groups.
Posture
Posture is defined as the attitude assumed by the body either with support during the course of muscular activity, or as a result of the coordinated action performed by a group of muscles working to maintain the stability. Posture is classified into two categories.
1. Dynamic posture is how one holds oneself when moving, For example, walking, running, or bending over to pick up something. It is usually required to form an efficient basis for movement. Muscles and non-contractile structures have to work to adapt to changing circumstances.
2. Static posture is how one holds oneself when stationary or not moving, For example, sitting, standing, or sleeping. Body segments are aligned and maintained in fixed positions. This is usually achieved by co-ordination and interaction of various muscle groups which are working statically to counteract gravity and other forces.
Extension Activity
Working in groups
• Distinguish between poor posture and proper posture.
• Describe proper posture while sitting, studying, writing, standing, walking.
• Discuss the significance of having a good posture.
Design a poster to be put up on the school Notice Board urging students to maintain good posture. Highlight the ill effects of poor posture.
It is important to make sure to maintain a good posture. This is possible where all body parts are aligned in such a way that least stress put on joints and muscles and, thus, it helps to prevent fatigue. A good posture helps to give good productivity in work, and leads to a physically and mentally stress-free condition. Postural deformity may be caused by heredity, disease, injury, poor habits, improper clothing, unhygienic living conditions, improper diet, improper exercises, lack of exercise, obesity, socio-economic status, etc.
Common Postural Deformities
There are a number of postural deformities, some of which are given below along with corrective measures. Corrective exercises should be done under advice and supervision of a physician or a physiotherapist.
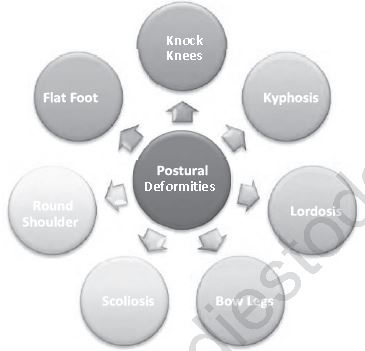
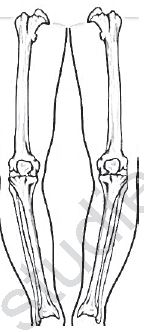
Knock Knees
Knock Knees, also known as Genu valgum, is a knee misalignment that turns the knees inward. As a result, both knees touch or knock against each other in a normal standing posture but there is a gap of 3-4 inches between the ankles. It is generally first noticed in early childhood, but in most cases, it usually corrects itself naturally by the time children are 7-8 years old. However, in some cases it continues till adolescence. In some cases Genu valgum can also develop due to an injury or infection in the knee or leg, rickets, severe lack of vitamin D and calcium, obesity, or arthritis in the knee.
It negatively effects walking and running and impedes other legs movement which hinder performance. In case Genu valgum persists beyond childhood, it may have other symptoms besides misaligned knees. They include stiff joints, knee pain and walking with a limp. Stressed ligaments and muscles can also cause pain in the hips, ankles, or feet. If only one knee is out of line, the stance may be unbalanced.
Do you know?
The man who discovered genes was an Austrian Gregor Mendel. Mendel was a scientist, Augustinian friar and abbot of St. Thomas' Abbey in Brno, Margraviate of Moravia. Though farmers had known for millennia that crossbreeding of animals and plants could favor certain desirable traits, Mendel's pea plant experiments conducted between 1856 and 1863 established many of the rules of heredity, now referred to as the laws of Mendelian inheritance.
Corrective Measures
Treatment for Genu valgum largely depends on the cause and severity of the problem. Exercises like horse riding and keeping the pillow between the knees and standing erect for some time are the best. For most people with Genu valgum, Yoga and exercise can help realign and stabilize the knees. Performing padmasana and gomukhasana regularly can help strengthen muscles of the legs and realign the knees. Strengthening exercises can be simple, such as leg raises while seated or lying down. Using of walking callipers is also a big help at pre-puberty stage.
Excessive body weight can be a contributing factor to Genu valgum as extra weight puts additional strain on the legs and knees, and this can cause knock-knees to worsen. A person who is overweight should lose weight through a combination of diet and exercise.
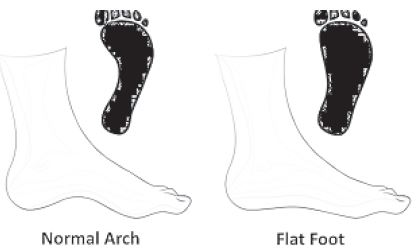
Flat Foot
Flat foot is also known as pes planus or fallen arches. It is a condition that may be diagnosed by looking at the arch of the foot or by taking the water print test. As the name flat foot suggests, people suffering from this deformity have either no arch in their feet, or one that is very low, allowing the entire soles of the feet to touch the floor in standing position.
Please click on below link to download CBSE Class 12 Physical Education Children And Women In Sports Notes
This problem may be genetic or environmental. At times a foot or ankle injury due to obesity, injury, wearing improper shoes (tight shoes, high heels etc.), carrying heavy weight for long time, arthritis or rheumatoid arthritis. It may be caused by a baby being forced to walk in an early stage, or it may be age related. Another condition that might cause flat feet is tarsal coalition.
This condition causes the bones of the foot to fuse together unusually, resulting in stiff and flat feet. Tightness in calf muscles may lead to temporary flat feet.
Arches provide a spring to the step and help to distribute body weight across the feet and legs. The structure of the arches determines how a person walks. Arches need to be both sturdy and flexible to adapt to stress and a variety of surfaces. When people have flat feet, it affects their posture while standing, their walking, running, and other related performances.
Flatfeet can sometimes contribute to problems in the ankles and knees. Majority of babies are born with flat feet but as they grow or get involved in physical activities the arch in the foot develops.
Corrective Measures
Exercises like walking, standing or jumping on toes and heels in all four directions, skipping rope, strengthens the muscles of foot which help to develop the arch in the foot. Activities like picking up marbles with toes, writing numbers in the sand with the toes will also help in developing the arch. Yoga asanas like Adhomukhsavasana performed in Surya Namaskar, Vajrasana and other therapeutic massages are also helpful in developing the arch.
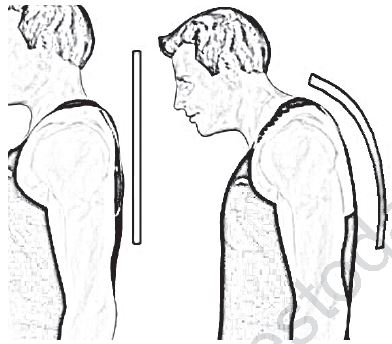
Round Shoulders
Round shoulders is a postural deformity in which shoulders are bent forward from the ideal alignment, thereby giving a narrow curve to upper back. It leads to postural deviations such as hyperkyphosis, or hunch back and anterior head carriage, or forward head posture. Over time, these postural conditions can progress and lead to other conditions such as chronic neck pain, thoracic outlet syndrome and lack of shoulder mobility.
It may occur at any age due to poor posture habits, heredity, muscle imbalance, tight fitting
clothes, injury, disease etc. Poor posture habits include using smartphone, tablet, computer, driving, carrying heavy weights and sitting for long periods.
Corrective Measures
Most important measure to correct rounded shoulders is strengthening and stretching of muscles and trying to correct the imbalance of muscles by doing chest stretches, T stretch, wall stretch, Handclasp stretch and planks, pull ups, reverse shoulder stretch, etc.
Developing the habit of keeping the spine straight is also helpful in correcting rounded shoulders. Yoga asanas like Chakrasana, Dhanurasana, can be useful in correcting rounded shoulders.
Kyphosis
Kyphosis is also known as Hunch Back or round upper back. The word Kyphosis comes from the Greek term kyph and means bent or bowed. It is a condition of the spine where the curvature of the upper back gets exaggerated or increases. It is an exaggerated, forward rounding of the back. Kyphosis can occur due to heredity, aging, disease (arthritis, osteoporosis), malnutrition, pulling of heavy weight over a period, unstable furniture, poor postural habit, weakness in muscles etc. It can occur at any age but is most common in older women. Age-related kyphosis is often due to weakness in the spinal bones that causes them to compress or crack. Kyphosis can appear in infants or teens due to malformation of the spine or wedging of the spinal bones over time.

While mild Kyphosis causes few problems, severe Kyphosis can cause pain and be disfiguring. This posture creates instability while walking, running etc. that may lead to fall or injury.
Corrective Measures
Exercises which help to strengthen back muscles, provide stability and make muscles more flexible should be performed. Physical therapy, swimming, exercise/ gym ball exercises, exercises with bands, and Yoga asanas like Dhanurasana, Chakrasana and Bhujangasana should be performed to get optimum benefits. Using a flat bed with a thin pillow while sleeping.
Lordosis
The term Lordosis comes from the Greek lordos which means bent backward. The spine curves a little in the neck, upper back, and lower back. These curves, which create the spine’s S shape, are called the kyphotic (upper back) and lordotic (neck and lower back).
Lordosis is a spinal deformity in which the angle of arc of the lower back is reduced. This leads to an increase and exaggeration of normal concavity of the lumber region of the spine.
It is also known as sway back. Chronic Lordosis may lead to pain and discomfort and become more serious if left untreated.

Lordosis is often caused by obesity, improper development of muscles, muscular or skeletal disease or accident, poor posture while standing, sitting and walking, malnutrition, etc. There are few cases where the cause was unknown. It is generally found in children because of weakening or tightening of muscles of the hip area, but they easily recover as they grow and muscles get strengthened.
Corrective Measures
Most people with Lordosis don’t require medical treatment unless it’s a severe case. In severe cases of Lordosis in children and teens may require use of braces, or even surgery.
Largely, weight loss, to help posture and daily physical therapy, to strengthen muscles and range of motion prove quite helpful. Exercises to develop strength in the pelvic region like sit-ups, sitting against the wall and pushing the trunk backward and lying on the back and raising upper extremities and legs together will give significant benefits. Yoga asanas including Dhanurasana and Halasana will be helpful. Use of braces, weight reduction, maintaining a good posture and taking a balanced diet are helpful in reducing the problem.
Scoliosis
The word Scoliosis comes from the Greek skolios which means bent. Scoliosis is a position in which the spine is tilted to either side of the body. It is a position of exaggerated lateral curvature or sideways curvature of the. In this disorder, the spine bends, twists or rotates in a way that it makes a C or an S shape. Scoliosis is found more commonly in girls than in boys and, though it can occur at any age, but it is more common during the growth spurt just before puberty. Most cases of scoliosis are mild, but some spinal deformities continue to get more severe as children grow. Severe scoliosis can be disabling. An especially severe spinal curve can reduce the amount of space within the chest, making it difficult for the lungs to function properly.

Scoliosis can be caused by conditions such as cerebral palsy and muscular dystrophy, or diseases like Arthritis, Paralysis, Rickets. It may result from lifting heavy weights, living in an unhealthy environment, and standing and sitting in a wrong posture. However, the cause of most scoliosis is unknown.
Corrective Measures
In cases of mild Scoliosis, no treatment is necessary. Some children may need to wear a brace to stop the curve from worsening. Others may need surgery to keep the problem from worsening and to straighten the spine. Exercises like hanging on the horizontal bars and swinging should be done on opposite side of the C-shaped curve. Aerobic activities with slow pace and breaststroke in swimming are helpful and also give good results. In yoga Trikonasana and Adhomukhasana should be performed to straighten the spine.
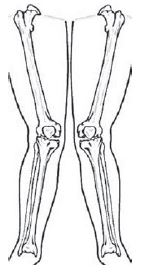
Bow Legs
Bow Legs, also known as Genu varum, is a position of knees in which legs look like a bow, when the legs curve outward at the knees while the feet and ankles touch. Infants and toddlers often have bow legs. It may be caused due to lack of Vitamin D, Phosphorus and Calcium and can be easily cured at an early stage. The condition doesn't cause pain or discomfort and is rarely serious. It does not affect running, standing, crawling etc. Bow legs is a condition that usually goes away without treatment, often by the time a child is 3–4 years old and does not affect a child's ability to crawl, walk, or run. However, parents might worry about the appearance of their child's legs, or an awkward walking pattern.
Sometimes, kids with bow legs may walk with the toes pointed inward, called pigeon-toes, or they may trip a lot and appear clumsy. Although in most cases the problem generally gets resolved on its own as the child grows, sometimes, it may lead to arthritis in the knees and hips. At times Bowlegs can be a sign of an underlying disease, such as Blount’s disease,
rickets, or arthritis.
Corrective Measures
Use of braces and modified shoes can be along with sufficient intake of balanced diet can prove to be of help. Walking on the inner edge of the feet may also help.
I. Tick the correct options
1. Deformity of the legs is known as
(a) Scoliosis
(b) Lordosis
(c) Knock knees
(d) Kyphosis
2. Lordosis is a problem of the
(a) Lower Back
(b) Middle Back
(c) Upper Back
(d) Shoulders
3. Scoliosis is a postural deformity related to
(a) Muscles
(b) Shoulders
(c) Legs
(d) Spine
4. Kyphosis is a deformity found in
(a) Shoulders
(b) Lumber region
(c) Hips
(d) Thoracic region
II. Answer the following questions briefly
1. What is meant by Round Shoulders? Mention a few exercises to correct it.
2. What is the Lordosis? Write in brief.
3. Write in brief the causes and symptoms of Knock Knees.
4. Explain corrective measures for Flatfoot.
III. Answer the following questions in 150-200 words
1. Explain any five postural deformities with their corrective measures.
2. Describe corrective measures of some common spinal postural deformities.
Participation of Women in Sports in India
Women's sports, both amateur and professional, have existed throughout the world for centuries in all varieties of sports. There is a rich record of sports participation of women in India. In the days of Mahabharata, Shakuntala, Madhuri, Kunti all choose physical activities as recreation. As time passed, India women were deprived of participation in sports for a number of reasons, despite having potential and talent. They were put on the back seat, and were not allowed to participate in sports. However, female participation and popularity in sports increased dramatically in the last quarter of the 20th century, reflecting changes that emphasize gender parity. Although the level of participation and performance can still be improved, women's participation in sports is generally accepted and promoted today.
Although women have shown a dramatic rise in sports participation, there is still a large disparity in participation rates between women and men remains. These disparities continue to hinder equality in sports. Many institutions and programmes still remain conservative and do not contribute to gender equity in sports. Some research in physical domain lists constraints like heavy limbs, pear-shaped body structure and postural deformities like flat foot knock knees etc., and physiological constraints including low level of RBCs, smaller heart and lungs, high fat percentage, menstrual disorders etc as reasons for women’s non-participation in sports. There are certain psychological constraints like low self-confidence and self-esteem, higher levels of stress and anxiety and social causes like lack of support or positive reinforcement from family and a male-dominated social structure that affect women’s participation in Sports. Religious and economic factors also play a negative role that affects women’s participation in sports

However, these constraints are now being reduced or eliminated as more women athletes are participating in sports. Regular physical activities and sports help to manage weight, tone the muscles, lower blood pressure, improve blood flow, increase high density lipoprotein and lower low density lipoprotein levels. Increased physical activity lowers the risk of heart and lungs disease and increases heart and lung capacity. Sports is an important tool for social empowerment and helps to develop skills like communication, teamwork, leadership, respect, social interaction, sportsmanship etc. and can significantly contribute to develop society and community. Sports participation not only provide health benefits but give overall development. Sport does not discriminate on the basis of colour, cast, creed, sex, race etc.
This trend of lower participation of women in sports exists not just in India, but is a global phenomenon. Participation of women at all levels from regional to international is limited. It affects all domains like participation in sports activities, administration of associations and federations, and participation in national and international level committees. Women who play sports continue to face many obstacles, such as lower pay, less media coverage, and different injuries compared to their male counterparts. Many female athletes have engaged in peaceful protests, such as playing strikes, social media campaigns, and even lawsuits to address these inequalities.
Do you know?
Some Indian women sportspersons who won medals in international events in 2019.
1. Dutee Chand - First Indian to win a 100m gold in a global event at the 30th Summer University Games in Napoli, Italy.
2. Hima Das - Won 5 gold medals in 20 days
• July 2, Poznan: 200m gold (23.65 seconds)
• July 7, Kunto: 200m gold (23.97 seconds)
• July 13, Kladno: 200m gold (23.43 seconds)
• July 17, Tabor: 200m gold (23.25 seconds)
• July 20, Prague: 400m gold (52.09 seconds)
3. PV Sindhu - First Indian to win World Championships
• 2013 - Bronze
• 2014 - Bronze
• 2017 - Silver
• 2018 - Silver
• 2019 – Gold
4. Manasi Joshi - Won BWF Para-Badminton World Championship Para-badminton player Manasi Joshi created history by securing gold at the BWF Para- Badminton World Championships, just a day before Sindhu.
5. PU Chitra - Clinched gold in women's 1500m race Won the Gold at the Asian Athletics Championship 2019 in Doha.
The International Olympic Committee (IOC) encourages participation not only in playing sports but in National Olympic Committees and International Federations and conducting regional seminars for female administrators, coaches, technical officials and journalists. In a recent announcement by IOC, 49% women will take part in next Olympic games. The constitution of India also provides gender equality and ensures to eliminate any type of hindrance. Sports is a medium to get gender equity and empowerment.
Constraints for Women's Participation in Sports in India
Physical Constraints - Physical constraints refer to the morphological feature adaptations to particular sports. Basically, it refers to the qualities of the sports person such as the physical fitness parameters. If there is failure in any of these required parameters it results in the reduction of sports performance. To mention a few: heavy musculature of limbs, pelvic or abdomen, improper posture/ postural deformity or flat foot.
Physiological Constraints - Physiological constraints refer to the organ functions ultimately impacting the system coordination. If there is any dysfunction of the organs it results in reduction of sports performance. Some women have lower levels of RBCs, lower percentage of Haemoglobin, smaller or weaker heart and it circulation, smaller or weaker lungs and breathing mechanism, dysfunction of organs of endocrine system, greater body fat percentage, dominance of neither aerobic power nor anaerobic power , Menstrual disorders.
Psychological Constraints - Psychological constraints comprise the behavioural process such as higher level of anxiety or aggression, lack of self- confidence, achievement motivation or interest, lower self-esteem or hesitation to participate during menstrual periods. These factors result in the reduction of wilful participation in sports.
Social Constraints - Social constraints refer to the behaviour of society in general and sports field in particular. During training and competition, the relationship with coaches, arena persons, training-mates, co-participants, opponents and officials during competition affects not just performance, but also participation. If there is any undue harassment or misbehaviour during this period, it results in reduction in sports performance or ultimately exit from sports participation. Lack of parental support and encouragement, and male dominant social structure also has a very negative impact on participation.
Religious Constraints - Religious constraints prevail in those societies who are fundamentalist and have rigid religious beliefs. They fear as society may ostracise them for going beyond the boundaries of their religion. This might also be the cause of limited participation in sports by women in India.
Economic Constraints - Economic constraints are considered the most important factor that hinders the women participation in sports. Insufficient funds, lack of sponsors also results in women exiting the sports arena. Economic constraints are magnified by the triangular or pyramidal factors. Non-availability of expert trainers, lack of sufficient infrastructural facilities and non-availability of sports equipment compounds the problem. Infrastructural facilities include availability of area for training, indoor stadiums or constructive sporting environment to undergo training. Lack of qualified coaches results not just in poor performance but also becomes a cause of sports injuries.
Because of the above discussed constraints and barriers women face problems is sports participation. Campaign for all women’s participation in sports should be encouraged in schools, colleges and in universities. Awareness programmes for women’s participation in sports should be conducted on a regular basis and they should be encouraged to participate in competitive sports. Families should also be encouraged to support their girls to participate in sports. Media coverage and sponsorship can enhance sports participation of women in India. Sports equipment must be developed focusing on physiological aspects of women. Appointment of women coaches, providing opportunities for competitions, eliminating cultural and social negativity and proper facilities can ensure larger participation. And in those states where religion is becoming a constraint should come up with some alternatives so that their women can also participate in sports and live a better and healthy life.
Now times are changing and society is accepting, and even encouraging, women’s participation in sports on National and International levels. In recent years, it has been raining gold on Indian women athletes in the International arena proving women are no less of a powerhouse when it comes to winning medals and championships for the country.
Barriers which prevented women from participating in sports are getting broken. Women are coming out and participating in sports and physical activities in large numbers. Karnam Malleswari was the first women who won a medal in Olympic Games in Sydney in 2000. In 2012, London Olympics, five times world champion Mary Kom won a medal in boxing and Saina Nehwal in Badminton. In 2016 Rio Olympics Sakshi Malik won medal in wrestling and P.V. Sindhu won the first ever women’s silver medal in badminton. P.T Usha and Anju Bobby George were athletes who earned a name in Athletics at international level. Our Indian women cricket team, wrestling, badminton, boxing, giving country name new heights.
I. Tick the correct options
1. Karnam Malleswari won a bronze medal in Olympic Games at
(a) Rio De Janeiro
(b) London
(c) Sydney
(d) Athens
2. Sakshi Malik won a medal in
(a) Badminton
(b) Weightlifting
(c) Wrestling
(d) Boxing
II. Answer the following questions briefly
1. Write a short note on benefits of participation in sports.
2. How has women’s participation in sports changed over the last two decades?
III. Answer the following questions in 150-200 words
1. Explain the various constraints faced by women in sports. How have they overcome them?
Menarche
The period of adolescence is marked by certain universal physical and biological changes in the body which lead to the attainment of sexual maturity. The time when sexual maturity is reached is called puberty. Menarche (first menstruation) is usually considered the point of sexual maturity for girls. It is the process in which female reproduction system matures and the body prepares itself for potential pregnancy. It is associated with the development of secondary sexual characteristics. Menarche is one of the most significant milestones in a woman's life. The average age for a girl to get her first period ranges from 8 to 15 years old.
Although the precise determinants of menarcheal age remain to be understood, genetic influences, socio-economic conditions, general health and well-being, nutritional status, certain types of exercise, seasonality, and family size possibly play a role. Over the past century the age at menarche has fallen due to reasons still unknown.
Menstruation (also termed as period or bleeding) is the process in a woman of discharging (through the vagina) blood and other materials from the lining of the uterus at about a monthly interval from puberty until menopause, except during pregnancy. This discharging process lasts about 3-5 days. Women usually have periods until about ages 45 to 55 and have menopause usually around age of 50. Menopause means that a woman is no longer ovulating and can no longer get pregnant. Like menstruation, age of menopause can vary from woman to woman and these changes may occur over several years.
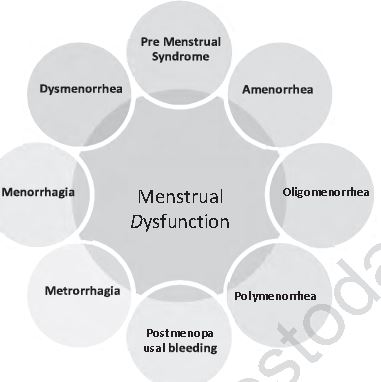
Menstrual Dysfunction
Menstrual dysfunction is an abnormal condition in a woman's menstrual cycle. Normal range of the menstruation cycle is 21 to 35 days. If it happens earlier than 21 days or after more than 35 days, then it’s a problem. Other menstrual problems include missing three or more periods, menstrual flow heavier or lighter in comparison with usual, cycle happening longer than seven days, any pain, cramping or vomiting during period, bleeding after menopause etc. Causes of abnormal menstrual cycles or menstrual order are: overweight, stress, dietary disorder, disease, sudden change in exercise schedule, travel, other medical complications etc.
There are different types of menstrual disorders which are given below:
1. Pre-menstrual Syndrome: Pre-menstrual Syndrome includes unpleasant or uncomfortable symptoms during the cycle. These may include depression, anxiety, irritation, headache, fainting, vertigo, infection etc. and may last from a few hours to few days. Symptoms Such symptoms may be reduced through moderate exercise, taking a balanced diet, having a good sleep and rest.
2. Amenorrhea: Amenorrhea is known as missed periods or absence of a normal monthly period or menstrual cycle. There are two types of amenorrhea.
(a) Primary amenorrhea: Menstruation cycle does not begin at puberty
(b) Secondary amenorrhea: It happens when menstruation for three months or more. This is the most common type of amenorrhea.
3. Dysmenorrhea: When menstruation happens with severe pain or frequent menstrual cramps, the condition is called Dysmenorrhea. Symptoms associated with dysmenorrhea may be cramping in lower abdomen, low back pain, pain in legs, nausea, fatigue, weakness etc.
4. Menorrhagia: Menorrhagia is characterized by heavy and long term or continuous menstrual bleeding.
5. Polymenorrhea: Polymenorrhea is a term used to describe a menstrual cycle that is shorter than 21 days.
6. Oligomenorrhea: Oligomenorrhea is infrequent menstruation. More strictly, it is menstrual periods occurring at intervals of greater than 35 days.
7. Metrorrhagia: Metrorrhagia refers to missed, delayed or erratic periods or abnormal bleeding patterns.
8. Postmenopausal bleeding: Postmenopausal bleeding is bleeding that occurs after one year of menopause or after a woman has stopped having menstrual cycles due to menopause.
The female hormones oestrogen and progesterone are important for overall body health. These hormones also regulate a woman’s periods. Intense exercise and extreme thinness can reduce the levels of these hormones to prevent or stop monthly menstrual cycles.
Extension Activity
Visit a nearby stadium and talk to women athletes. Collect a data of 5 such athletes in their teens. Are they facing any problem related to their health, diet etc? Discuss about it in the class.
I. Tick the correct options
1. Frequent menstruation is known as:
(a) Metrorrhagia
(b) Oligomenorrhea
(c) Polymenorrhea
(d) Menorrhagia
Answer : C
2. If the menstruation cycle does not begin at puberty, the condition is called
(a) Primary amenorrhea
(b) Secondary amenorrhea
(c) Oligomenorrhea
(d) Dysmenorrhea
Answer : B
II. Answer the following questions briefly
1. What is menstrual dysfunction? Write in brief.
2. Explain the term Menarche.
3. Write short note on Amenorrhea.
III. Answer the following questions in 150-200 words
1. Explain menstrual dysfunction.
Female Athlete Triad
Participation in sports and physical activities provides a lot of physical and social benefits like developing leadership qualities, competition, team work etc. Regular participation in such activities is associated with a longer and better quality of life, reduced risks of a variety of diseases and many psychological and emotional benefits. Evidence suggests a positive relationship between physical activity and a host of factors affecting girls’ physical health, including diabetes, blood pressure and the ability to use fat for energy, thus preventing obesity. Physical activity could reduce the risk of chronic diseases in later life. Conditions, such as cancer, diabetes and coronary heart disease, have their origins in childhood, and can be aided, in part, by regular physical activity in the early years. Also, regular activity beginning in childhood helps to improve bone health, thus preventing osteoporosis, which predominantly affects females.
However, participation in sports is not without certain health risks. Sports like Judo, boxing, wrestling, taekwondo etc. exert a lot of pressure on athletes to maintain their shape and weight. Participation in sports like distance running, cycling, cross country etc. athletes have to take a balanced diet since these demand high levels of energy and a good quantity of dietary intake. Such pressures put the athlete’s health at risk and leads to Female Athlete Triad. The term ‘triad’ was first described by American college of sports medicine in 1992, and the three components to describe the triad were
(a) disordered eating,
(b) amenorrhoea and
(c) osteoporosis
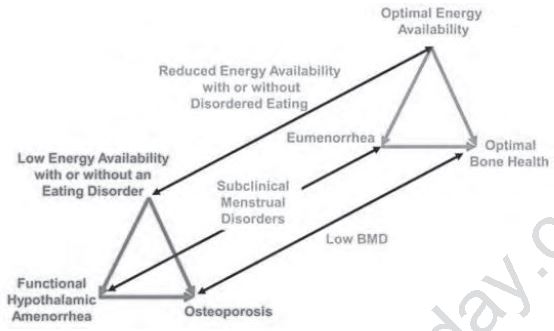
Picture Source 4
The illustration above depicts the female athlete triad spectrum. The black lines represent the spectrums of each of the 3 components and the red and green triangles show both of the extremes. The top green triangle represents a healthy athlete who has a good balance between energy intake and expenditure. Because of this, they have a normal menstruation cycle and a bone mineral density that is above average for the athlete’s age. The bottom left, red triangle represents an athlete who does not have an appropriate balance between energy intake and expenditure, which may be the result of restrictive dieting and/or clinical eating disorders.
The terms to describe Female Athlete Triad have now been revised. The new terms to indicate problems are
(a) low energy availability with or without eating disorder,
(b) dysfunction of menstruation and
(c) low bone density.
This change was relevant because all these three revised components can be easily resolved by proper energy intake and expenditure and same may be used as effective strategy. Thus, if an individual takes optimum calories as required by body, including energy required for physical activity and energy required for body functions, the result is promotion of healthy bones and normal menstrual function. All three components are very much interlinked.

Low Energy Availability with or Without Disordered Eating
Disbalance of energy may occurs due to disordered eating and eating disorderly. The problem of female athlete triad originated from not balancing energy intake and energy expenditure. Consequently, an athlete must have knowledge of how to balance the energy intake.
Eating disorder is known as gross disturbance in eating behaviour. Disordered eating has wide range of harmful and often ineffective eating behaviours in the process of weight reduction.
These includes calorie restriction to clinical disorders of Anorexia nervosa and bulimia nervosa. Sportspersons participating in activities in which leanness or specific weight is required for performance are at higher risk of developing eating disorders. Coaches, team physicians, parents, and other supporting staff should know the symptom so that the problem can be treated on time, other-wise it leads to long term physiological, psychological effects or, in extreme cases, fatal results.
Anorexia nervosa is an eating disorder where an individual tries to reduce body weight abnormally, having an intense fear of gaining weight or misconception over his/her weight.
Individuals with anorexia place a high value on controlling their weight and shape, using extreme efforts that tend to significantly interfere with their lives. To prevent weight gain or to continue losing weight, people with anorexia usually severely restrict the amount of food they eat. They may control calorie-intake by vomiting after eating or by misusing laxatives, diet aids, or diuretics. They may also try to lose weight by exercising excessively. No matter how much weight is lost, the person continues to fear weight gain. Symptoms may include menstrual dysfunction, constipation, diarrhoea, bloating, unexpected weight loss, muscle weakness, stress fracture, bone weakness, overuse injuries, anxiety etc.
Bulimia nervosa is an eating disorder in which an individual eats large amount of food with loss of control over eating and then adopts unhealthy ways to cut down calories like vomiting, take laxatives, weight loss supplements, diuretics, excessive exercises etc.
Symptom of bulimia are dehydration, dental problems, oedema, electrolyte abnormalities, extreme weight fluctuation, menstrual irregularity, weakness, cramps, depression etc.
Menstrual Dysfunction
Menstrual irregularities is one of the components of Female Athlete Triad and it is a marker of quality health in female athletes. Menstrual dysfunction is common in sportswomen and is often ignored. It is important that young female athletes should be informed enough to understand the problem and must know the management of the menstruation disorder. If the problem is managed in time, then it may positively affect athletic performance. Ignored or untreated menstrual irregularities may have a prolonged effect on bone mineralization and the treatment may last months and years. Generally female sportspersons suffering from menstrual irregularities, self- select different sports in comparison with normal menstruating peers because in delayed puberty females develop strong bones and taller height than others. However, such dysfunction may affect sports performance in the long run and lead to complications. Recent research says weight training has lots of benefits including strengthening of the bones and may not affect adolescent menstrual irregularities. Studies show that more than 15% females participating in Olympics may be suffering from amenorrhea. Sometimes the skeletal health of a female athlete suffering from amenorrhea is much lower than that of a sedentary woman.
Low Bone Mineral Density
Low bone mineral density, previously termed osteoporosis, may be defined as a disease marked by increased bone fragility, disturbance in bone structure including low bone mineral density (BMD) that may result in fractures, pain, deformity, disability etc. Low BMD is generally caused by improper diet and amenorrhoea. Due to low level of oestrogen and progesterone in female athletes, their bones become weaker and lose minerals. Effects of low bone mineral density include increased occurrence of injury, stress fractures, and risk of early osteoporosis after menopause. Deposition of bone increases during childhood and adolescence and peaks during the 20s and 30s. A large genetic component to BMD also exists, with heritability of BMD suggested to be 50–85%. Knowledge of family history or other medical condition linked with BMD will help keep female athletes safe from risk of injury and fractures. Intensity, volume, frequency, type of activity should be determined by knowledge of genetic characteristics.
The female athlete triad is a result of energy imbalance; thus, adjusting the energy expenditure and energy availability is the main intervention. For this the main treatment is restoration of regular menstrual cycle for reestablishment of energy balance and enhancement of bone mineral density. The strongest predictor of recovery to normal menstrual function in young athletes is weight gain. Family-based therapy and cognitive behavioural therapy, also have been known to be effective interventions for disordered eating. A sports nutritionist can help the athlete and her family determine the quantity and quality of food consumption and dietary supplements required to meet her bodily functions, replace energy output due to athletic training, and enhance bone health. Additionally, weight gain may be necessary to increase BMD.
Case Study
In 2000 Sydney Games weightlifter Karnam Malleswari won the bronze medal and created a historic moment for India, becoming the first Indian woman to win a medal at the Olympics. She was followed by Saina Nehwal and Mary Kom in the London Olympics 2012 years. the Olympics. The last eight years have seen a slow, but steady rise for Indian women athletes at world events. Study the charts given below and answer the following questions?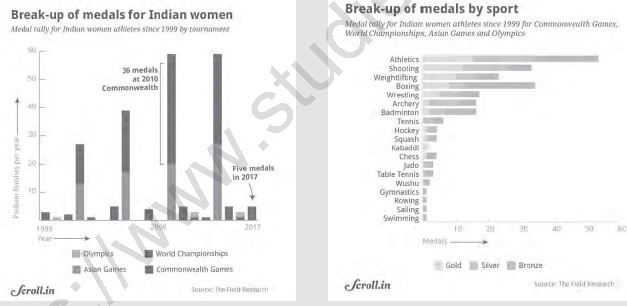
Picture Source 5
Q. Which year marks a turning point in women’s winning medals at International Sports Competitions?
Q. Which are the fields that they have excelled in?
Q. In which International competition have they won the greatest number of medals?
Q. What are the reasons for the consistently good performance of Indian women in International sports?
I. Tick the correct options.
1. Weakening of bones due to loss of bone density and improper bone formation is
(a) Amenorrhea
(b) Anorexia Nervosa
(c) Osteoporosis
(d) Lordosis
2. What is the cause of Osteoporosis in women?
(a) High blood pressure
(b) Menarche
(c) Excessive exercise
(d) Lack of calcium and vitamin D
3. Female athlete triad is a syndrome characterized by
(a) Osteoporosis
(b) Amenorrhea
(c) Eating disorder
(d) All of the above
4. In which type of Anorexia does an individual lose weight by taking laxatives or diuretics
(a) Bulimia Nervosa
(b) Purging type
(c) Restricting type
(d) Anorexia Nervosa
II. Answer the following questions briefly.
1. Explain eating disorder.
2. Write a short note on Bone Mineral density.
III. Answer the following questions in 150-200 words
1. What is Female Athlete Triad? Explain.
CBSE Class 12 Physical Education Children And Women In Sports Notes
Students can use these Revision Notes for Children And Women In Sports to quickly understand all the main concepts. This study material has been prepared as per the latest CBSE syllabus for Class 12. Our teachers always suggest that Class 12 students read these notes regularly as they are focused on the most important topics that usually appear in school tests and final exams.
NCERT Based Children And Women In Sports Summary
Our expert team has used the official NCERT book for Class 12 Physical Education to design these notes. These are the notes that definitely you for your current academic year. After reading the chapter summary, you should also refer to our NCERT solutions for Class 12. Always compare your understanding with our teacher prepared answers as they will help you build a very strong base in Physical Education.
Children And Women In Sports Complete Revision and Practice
To prepare very well for y our exams, students should also solve the MCQ questions and practice worksheets provided on this page. These extra solved questions will help you to check if you have understood all the concepts of Children And Women In Sports. All study material on studiestoday.com is free and updated according to the latest Physical Education exam patterns. Using these revision notes daily will help you feel more confident and get better marks in your exams.
FAQs
You can download the teacher prepared revision notes for CBSE Class 12 Physical Education Children And Women In Sports Notes Set 01 from StudiesToday.com. These notes are designed as per 2026-27 academic session to help Class 12 students get the best study material for Physical Education.
Yes, our CBSE Class 12 Physical Education Children And Women In Sports Notes Set 01 include 50% competency-based questions with focus on core logic, keyword definitions, and the practical application of Physical Education principles which is important for getting more marks in 2026 CBSE exams.
Yes, our CBSE Class 12 Physical Education Children And Women In Sports Notes Set 01 provide a detailed, topic wise breakdown of the chapter. Fundamental definitions, complex numerical formulas and all topics of CBSE syllabus in Class 12 is covered.
These notes for Physical Education are organized into bullet points and easy-to-read charts. By using CBSE Class 12 Physical Education Children And Women In Sports Notes Set 01, Class 12 students fast revise formulas, key definitions before the exams.
No, all study resources on StudiesToday, including CBSE Class 12 Physical Education Children And Women In Sports Notes Set 01, are available for immediate free download. Class 12 Physical Education study material is available in PDF and can be downloaded on mobile.